
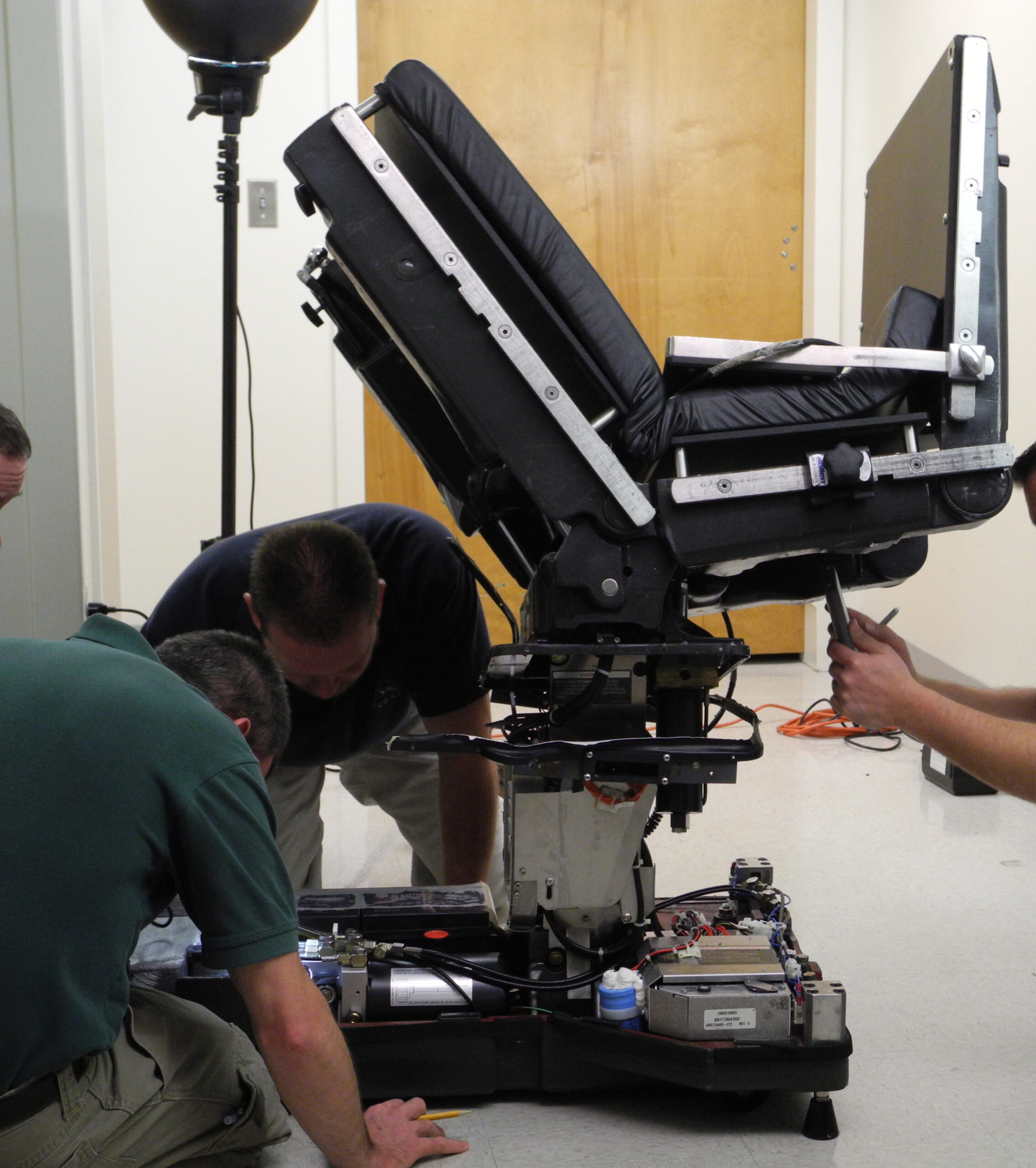
 In this case, a patient was lying fully anesthetized on an OR table for a surgical procedure. Several minutes into the procedure, the table began to move without being directed by OR personnel. Efforts to stop the movement by using the standard control pendant or over-ride switches were unsuccessful. The table continued to move even after the power cord had been unplugged from the electrical receptacle. Eventually, the head and foot sections folded up to their extreme positions and the table tilted fully to one side, as shown in the adjacent photograph. The patient received severe injuries.
In this case, a patient was lying fully anesthetized on an OR table for a surgical procedure. Several minutes into the procedure, the table began to move without being directed by OR personnel. Efforts to stop the movement by using the standard control pendant or over-ride switches were unsuccessful. The table continued to move even after the power cord had been unplugged from the electrical receptacle. Eventually, the head and foot sections folded up to their extreme positions and the table tilted fully to one side, as shown in the adjacent photograph. The patient received severe injuries.
Issues
The immediate issue from a forensic engineering perspective was to determine the proximate cause of the uncontrolled movement. Related concerns were why the movement could not be stopped by use of the control pendant, by use of the over-ride switches, or by unplugging the table.
Following a determination of the proximate cause, the focus shifted to the underlying factors that may led to the proximate cause and may have contributed to the incident.
Discussion
A detailed examination of the physical condition of the table — without touching, manipulating, or powering the table — was carried out by engineering experts associated with all parties to the lawsuit. The table was in generally good physical condition except for damage to the outermost shroud of the telescoping support column and associated damage to adjacent bank of over-ride switches.
The engineering experts then began to step through a detailed testing protocol that had been developed earlier. No steps were taken without consensus among the experts. Photographic documentation was made at every step. Written notes taken by any expert were later copied and made available to all other experts.
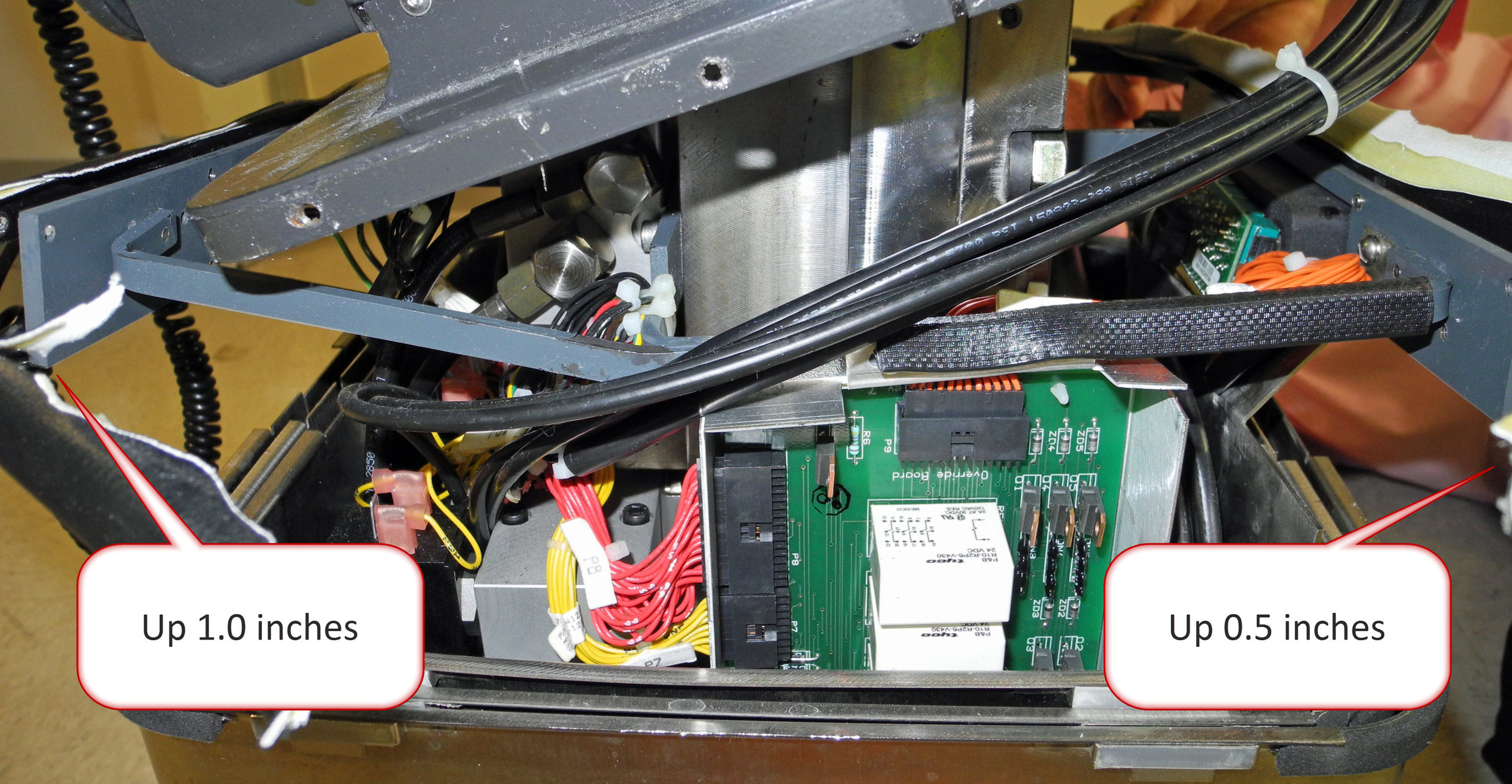
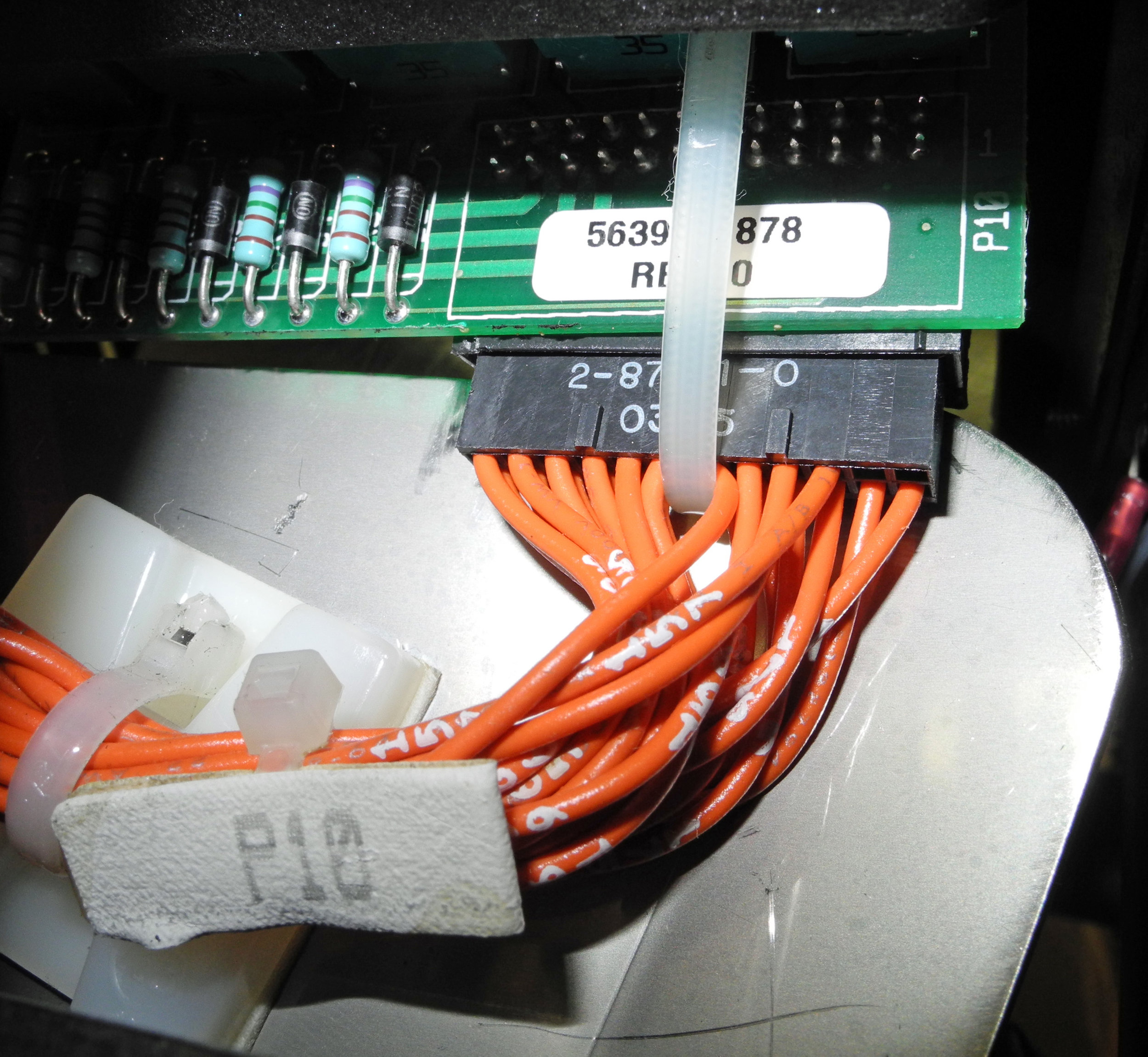
The early steps in the testing protocol were primarily disassembly of the OR table and observation of what each step revealed. Some steps involved electrical measurements and limited application of power to the table. Refer to the photo gallery below for visual details.
The proximate cause of the uncontrolled movement was determined to be internal damage the some of the over-ride switches. Some of the damage was apparent visually and some of it could be determined only through measurement of electrical characteristics. The damaged switches effectively called for the table to move on multiple axes toward the final observed configuration. The movement did not end until the components of the bed reached their mechanical limits.
Why was it not possible for the control pendant to stop the motion? By the table’s design, the physical over-ride switches supersede the signals of the control pendant.
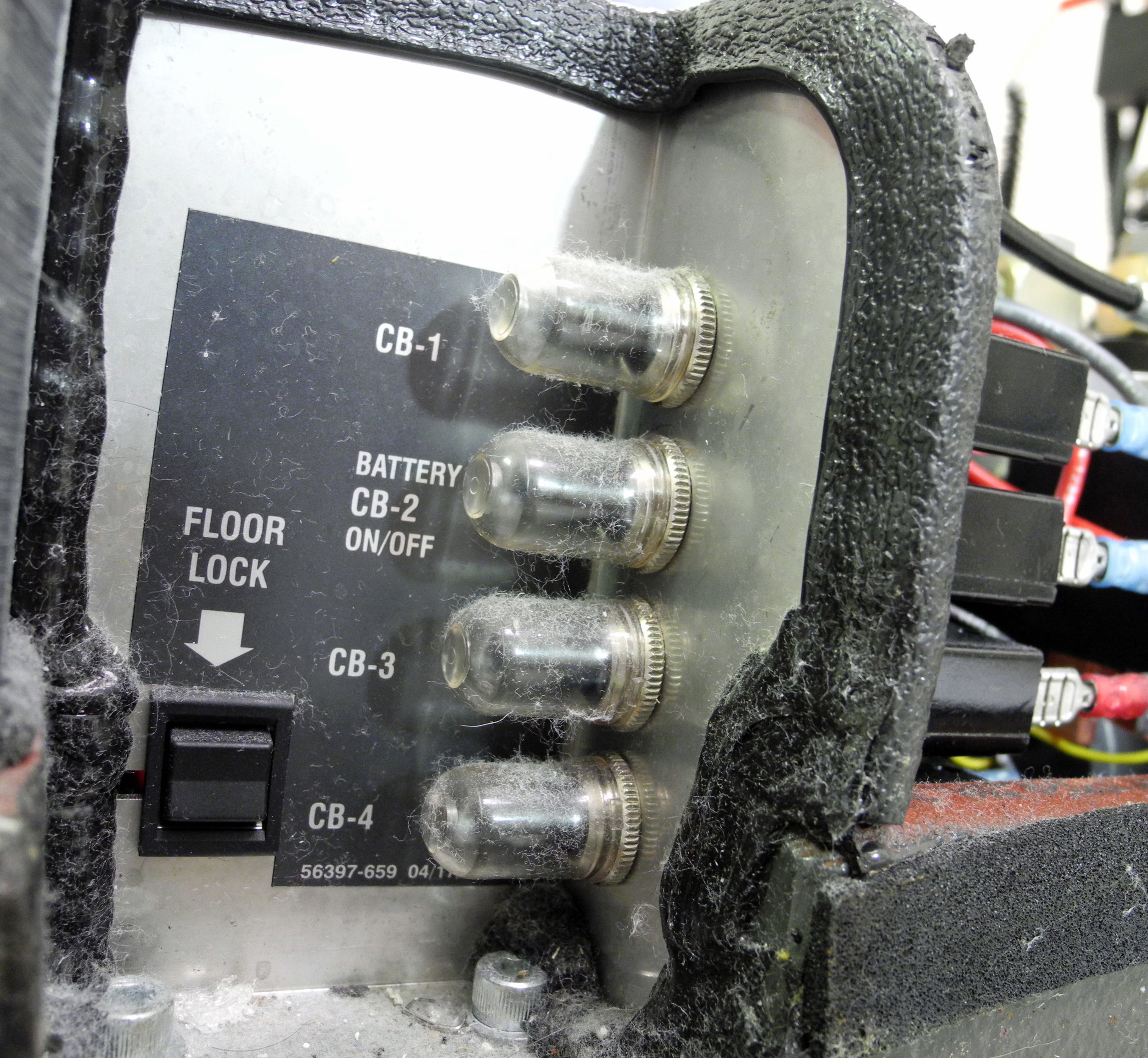
Why did unplugging the table not stop the motion? The base of the table includes a bank of batteries that allow the patient position to be adjusted in the absence of electrical power. This fact raised additional issues: Why was there no “emergency stop” control on the table? Were OR staff adequately trained on how to respond to this type of situation?
How did the over-ride switches get damaged? It was possible to identify the sequence of mechanical events that led to physical damage. However, the more important issue was how that sequence of events came about. Could the table have been designed to make these events less likely? Could “use error” have contributed to the incident. Could better maintenance have averted the incident.
Forensic Engineering Considerations
This case illustrates the importance of establishing a testing protocol well ahead of actual testing and with agreement by all parties. That lets testing proceed steadily without the need to stop at every point to decide how to move forward. However, the protocol should also identify decision points at which the test findings can determine which of two or more paths forward is appropriate.
It also shows the value of joint testing by multiple experts. It promotes data-sharing during the discovery phase. There are also cases in which no single party has all of the testing capabilities relevant to the case. For example, in some cases the medical device manufacturer is the only party with specialized test fixtures.
An important concept to keep in mind is “use error.” What it means is that someone was using a medical device to achieve a clinical objective — diagnosis, treatment, monitoring — but was unable to achieve it. The concept of “use error” is distinct from “user error” because it does not assume that the user is to blame. It leaves open the question about which of the many possible explanations contributed to the incident.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}